If patients with erectile dysfunction do not respond to oral or topical medications, the next step would be consider trying a vacuum pump device, which draws blood into the penis by creating a negative pressure around the penile shaft (Fig. 1). Once the penis becomes erect, a compression ring is applied at the base of the penis to prevent blood from draining out, and must be removed after sexual intercourse is completed.

As a last resort, patients may consider surgery to insert a prosthetic penile implant (Fig. 2). This procedure involves insertion of an inflatable implant device in the penile shaft, which creates an erection by fluid flowing into the device from a concealed reservoir placed beneath the skin. Advantages of such penile implants include the consistency of good erections achieved and control of the duration of erection.

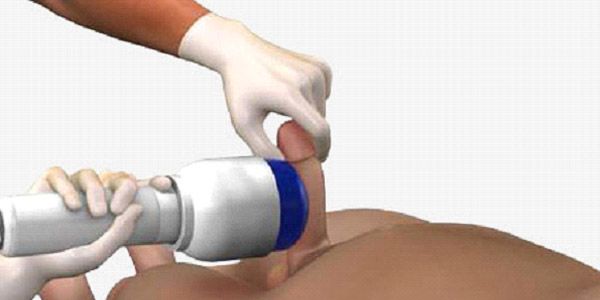
Yes! In recent clinical trials, low-intensity shockwave therapy (LIST) to the penis has recently been found to be an effective treatment for patients with erectile dysfunction that are not responsive to oral medications. In this treatment, focused shockwaves of low intensity are targeted at the smooth muscle in the penis, causing mechanical shear stress and microtrauma (Fig. 3). This causes the body to produce chemicals to improve blood flow and stimulate new vessel formation (angiogenesis) to the cavernosal tissue in the penile shaft. Current treatment protocols comprise 6 sessions lasting 15-20minutes each, over a 3-week period, where shockwaves are administered to the penis. Whilst several patients report an improvement in erectile function, the response may wane over time and repeat treatment may be required4. Shockwave therapy for erectile dysfunction is now available in Singapore, and our early experience with this novel treatment has been very encouraging.