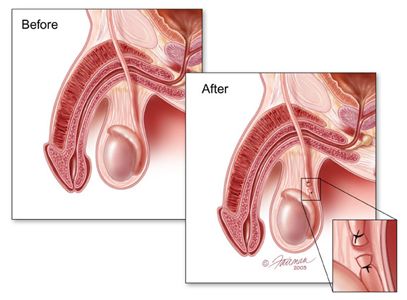
The vasa deferentia are tubes which carry viable sperm produced in the testicles to the male urethra, which are discharged together with seminal fluid from the seminal vesicles to form the semen at time of ejaculation. During a vasectomy, the vas deferens on each side is identified, delivered through a small incision in the scrotal wall and divided, thereby disrupting the delivery of viable sperm out of the body. The cut ends of the vas deferens are tied off with sutures, and one of the ends may be covered by the layers of overlying tissue to minimize the possibility of the severed ends restoring continuity in the future (known as fascial interposition).
Innovations in surgical techniques for vasectomy have included (1) no-scalpel vasectomy (NSV), in which the surgeon uses a sharp pointed forceps to puncture the scrotal skin and deliver the vas deferens; (2) use of fascial interposition; and (3) use of cautery to occlude the severed ends of the vas deferens. These techniques have been validated in several studies to improve the success rate of achieving azoopsermia (the absence of viable sperm) after surgery.