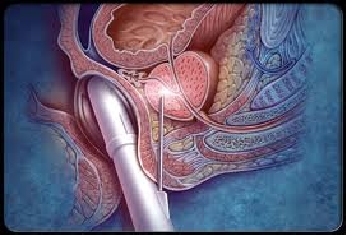
Prostate cancer usually occurs in men aged over fifty years, and becomes more common as men get older. In its early stages, prostate cancer does not cause any symptoms. It is usually detected on finding an abnormally raised serum prostate specific antigen (PSA) level, followed by an ultrasound-guided needle biopsy to confirm or exclude the presence of cancerous cells in the prostate (Fig. 2). With PSA blood tests becoming easily accessible over the last twenty years, the majority of men with prostate cancer are now diagnosed at an early curable stage of their disease. In its advanced stages, prostate cancer may cause obstruction to the urethra with difficulty passing urine; frank blood in the urine (haematuria); blood in the semen (haematospermia); or painful urination. If the cancer has spread to the bony skeleton, patients may experience pain in the back or hips.
Early prostate cancer is an imminently curable disease, and usually carries a very good prognosis if it is detected before the cancer has extended outside the prostate gland. The conventional treatment options are (1) surgery to remove the prostate gland if patients are less than 70 years of age and in good health – in Singapore, this is routinely performed through small incisions using the da Vinci robot (Fig. 3); (2) radiation therapy to ablate the cancer cells in the prostate (Fig. 4); or (3) active surveillance in certain patients whose cancer characteristics have a very low risk of progressing or spreading. For patients choosing curative treatment with surgery or radiation, common side-effects include urinary incontinence (usually a short-lived phenomenon) and impotence.


Most international guidelines recommend active surveillance as a treatment option for patients with clinically confined prostate cancer that has very low risk of cancer progression2,3. The strict criteria for such patients include:
- Life expectancy of more than 10 years
- Clinical stage T1/T2 cancers (ie. prostates with no or very small palpable nodules)
- Serum PSA < 10ng/dl
- Gleason prostate biopsy score of ≤ 6 (out of 10)
- ≤ 2 positive cores on biopsy (minimum of 12 cores taken)
- ≤ 50% cancer involvement per biopsy core
In addition, a consensus meeting recently suggested excluding men from active surveillance if their prostate biopsy reports contained any of the following worrisome characteristics: (1) predominant ductal carcinoma; (2) sarcomatoid carcinoma; (3) extraprostatic extension of cancer; and (4) lymphovascular invasion3 (Fig. 5).
