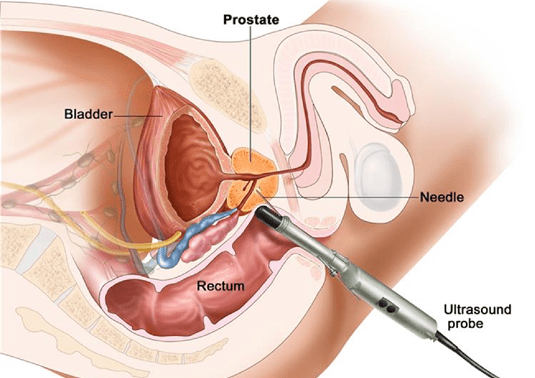
Most urologists perform a prostate biopsy using a transrectal ultrasound probe (Fig 1). This short procedure is performed in the clinic or day surgery centre, usually under mild sedation for patient comfort. The patient is requested to lie on his side, and the rectum is cleansed with an antiseptic solution. A transrectal ultrasound probe is then inserted into the rectum under lubrication, and images of the prostate gland are taken. Local anaesthetic is administered to the nerves running alongside the prostate gland, and twelve or more cores of the prostate are taken with ultrasound guidance using a quick-firing needle. After the biopsy is completed, the urologist will check for any bleeding from the rectum, and if necessary place a gauze or inject some medicine to the bleeding points. The patient is then woken up, and asked to consume a few cups of fluid. Once he is able to pass urine, he may be discharged and a date given for him to return to discuss the prostate biopsy report, which usually takes less than a week to be finalized.
In the overwhelming majority of patients, transrectal ultrasound-guided (TRUS) biopsies of the prostate are safe and uneventful. Whilst uncommon, possible complications include (1) persistent bleeding from the rectum; (2) difficulty passing urine after the biopsy (urinary retention); and (3) severe infection (known as sepsis) from bacteria being translocated from the rectum into the prostate (Fig 2). The incidence of TRUS-biopsy sepsis is relatively low (<5%), but should be always be suspected if patients develop fever, chills, sweats, or lethargy after the procedure. When detected early, patients with TRUS-biopsy sepsis often recover within a few days with prompt hospital admission and treatment with broad spectrum intravenous antibiotics and supportive medications.

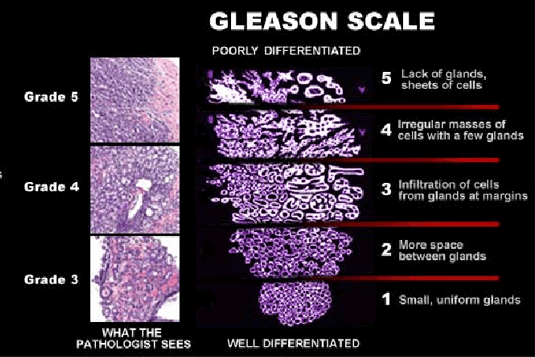
When the prostate biopsy cores are sent to the laboratory, the pathologist will stain them for examination under the microscope to look for evidence of cancerous change to the architecture of the prostate gland. If present, the pathologist will then assign a Gleason score from 2 to 10 to describe the aggressiveness of cancerous change in the prostate (Fig.3). Prostate cancers with a Gleason score of 6 or below are usually considered indolent or low risk, whilst those with a score of 8-10 are deemed highly aggressive and mandate early definitive treatment.
Should your prostate biopsy report confirm the presence of cancerous change, your urologist will advise you to proceed with tests to accurately stage the extent of prostate cancer spread. These will involve (1) magnetic resonance imaging (MRI) scan of the prostate, to see if the cancer has spread outside the capsule of the prostate gland and / or involved the nearby lymph nodes, and (2) a whole body bone scan to see if the cancer cells have spread to the bony skeleton (Fig. 4). Based on how early or advanced the stage of prostate cancer is, your urologist will then advise you on the most appropriate treatment available in your region.
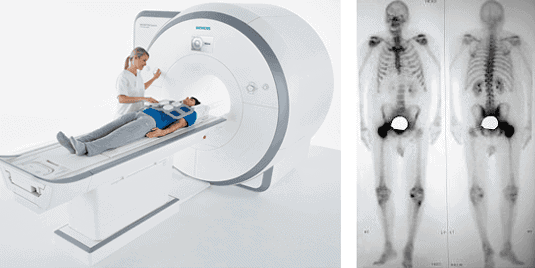 Fig 4. Staging of prostate cancer is usually assessed with (A) Magnetic resonance imaging of the prostate gland and (B) Bone scan.
Fig 4. Staging of prostate cancer is usually assessed with (A) Magnetic resonance imaging of the prostate gland and (B) Bone scan.
Fig 4. Staging of prostate cancer is usually assessed with (A) Magnetic resonance imaging of the prostate gland and (B) Bone scan.